Chondromalacia of the Knee
Post Operative Instruction After Arthroscopy
The word “chondromalacia” means cartilage (chondro) softening (malacia). This may occur in any joint but is commonly used to describe surface changes of the knee cap (patella). Patellar chondromalacia truly describes cartilage changes seen microscopically but has been generalized to encompass the clinical condition. The patella, or kneecap, is an oblong bone which is embedded within the extensor tendon of the knee. The patella increases the leverage of the extensor muscles (quadriceps) and acts also as a pulley, around the femoral groove. Both the patella and the femoral groove which it contacts, have smooth cartilage surfaces lubricated by synovial fluid (joint oil). The cartilage also absorbs enormous loads during daily activities. Walking on level ground exerts a contact force of one-half body weight. Climbing stairs increases the force to four times body weight. Arising from a squat can generate patellar forces up to eight times body weight. Chondromalacia may occur as a result of a direct blow to the patella, fracture or patellar dislocation, or more commonly, over a period of years because of wear and tear. Patellar arthritis then develops because of patellar maltracking. This occurs because of overuse, coupled with anatomic malalignment and supporting soft tissue imbalance. The anatomic factors responsible for the alignment and patella tracking are tibiofemoral angle (knock-knee or bow-leg), tibiofemoral rotational alignment, patella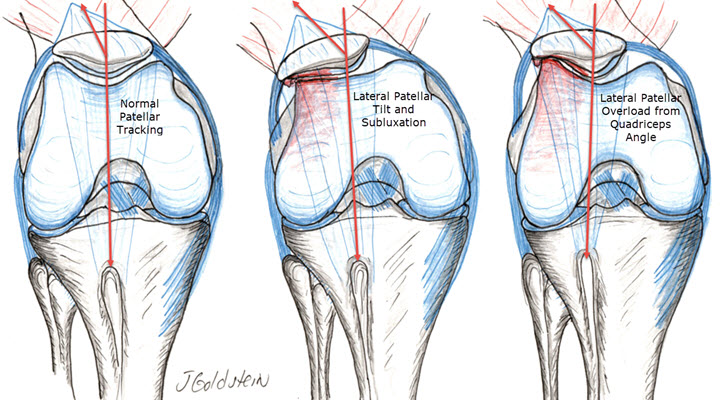 r and femoral groove shape and congruity, and capsular and muscular balance. In general, maltracking from any cause exposes the cartilage of patella and femur to localized excessive load and accelerated wear. The condition is more common in women and is frequently seen during adolescence. It is often associated with activities which induce high patella-femoral loads such as hill-climbing, cross-country running, jumping, and squatting.
r and femoral groove shape and congruity, and capsular and muscular balance. In general, maltracking from any cause exposes the cartilage of patella and femur to localized excessive load and accelerated wear. The condition is more common in women and is frequently seen during adolescence. It is often associated with activities which induce high patella-femoral loads such as hill-climbing, cross-country running, jumping, and squatting.
SYMPTOMS
Symptoms are fairly nonspecific but the history is relatively diagnostic. Pain is generally dull, aching and generalized to the “front” of the knee. Pain occurs with, or more commonly, hours or days after aggravating activities. There is often mild swelling noted after aggravating activities. Cracking, popping or grating is both palpable and at times audible when flexing and extending the knee. Prolonged sitting often results in aching and stiffness. The pain is experienced in the bone which feels abnormally high pressure against it. The consequence of abnormal pressure is accelerated wear. The debris generated leads to inflammation, swelling, and pain.
DIAGNOSIS
Diagnosis is made primarily by direct visualization. No one test is diagnostic, however, careful examination and evaluation result in high diagnostic accuracy. Plain X-ray examination is often suggestive and sometimes diagnostic of malalignment or abnormal wear. Specialized exam such as CT scan or MRI are generally not indicated except in instances where another pathology is suspected. Although chondromalacia is an early form of arthritis, it rarely results in severe disabling symptoms and has no relationship to generalized arthritis. Typically, the patient experiences ups and downs in symptoms related to their activities.
TREATMENT
Orthopedic treatment is aimed at reducing the regularity and severity of symptoms. This may be accomplished by avoiding or modifying aggravating activities and lowering body weight. Over time, the patella and femoral surfaces will then smooth out the rough areas. An exercise program which strengthens the quadriceps muscles (extensors) and stretches the hamstrings helps to balance the forces holding the patella central in the femoral groove. A strong quadriceps also dampens forces the surface cartilage sees by absorbing more energy of acceleration and deceleration. Short-arc extension exercises especially laying partly toward the affected side, and straight leg raising also in this position, are helpful early exercises. Stairmaster (with short rapid steps), mini-squats, a bicycle with a light load and the seat raised high, and pulling yourself in a rolling desk chair by your feet on the ground, are all helpful exercises. Icing the knee for 20 minutes after aggravating activities and short courses of aspirin or other anti-inflammatory medications may be beneficial. A patella “brace” or sleeve may aid symptoms of mild maltracking. Swimming and cycling (straight line exercises) are best tolerated, but the guide to activity should be pain and swelling.
REHABILITATION
Rehabilitation is very dependent on the Orthopedic procedure necessary. Please see After Arthroscopy for information. Arthroscopic lateral release (dividing the lateral knee capsule) although simple and quick to perform, requires a long period of rehabilitation to regain the strength of the extensor mechanism and improve stability. This typically will not work by itself in patients with a very high Quadriceps angle. Swelling of the knee, especially after activities which load the extensor mechanism, may take 4 months to resolve even after simple lateral release. More extensive realignment procedures which move the patellar tendon site of attachment, require healing of the bone attachment site as well as surrounding soft tissue healing. Here improvements may be expected 4 to 6 months following surgery. Much of the necessary rehabilitation may be undertaken on a home program of therapy or at a gym facility, once the required exercise program is familiar and progress is made to a safe and comfortable point after surgery.
Compliments of Sports Medicine and Orthopaedics, East Providence, RI