Deep Venous Thrombosis
Deep venous thrombosis is a serious complication following lower extremity surgery or following serious trauma. This can lead to pulmonary embolus when a clot flows into the lung and blocks some of the normal flow. These clots in the deep veins of the lower extremities are common below the knee and less common higher up where they are more concerning. People who are overweight are more likely to have this complication. In addition, patients with some clotting disorders can be very prone to deep venous thrombosis. In general, patient activity is a contributing factor. A rapid return to ambulation and normal function likely lowers the risk of deep venous thrombosis dramatically.
Symptoms: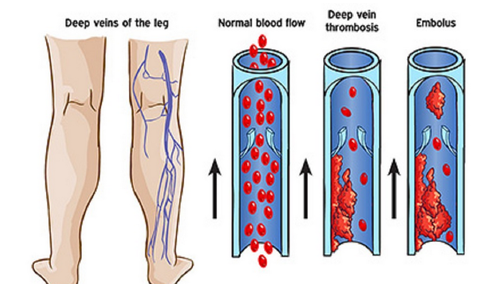
Symptoms often begin with increasing swelling in the affected extremity. This may be difficult to discern from normal swelling which occurs following surgery itself. In general, early deep venous thrombosis does not cause increased pain only swelling. In the case of pulmonary embolus, patients often become short of breath and have difficulty ambulating more than short distances. This is, fortunately, a fairly rare complication occurring in only a small fraction of patients with deep venous thrombosis. Prophylaxis lowers the risk of any of these complications dramatically.
Diagnosis:
Typical diagnosis is made beginning with a physical exam, however, this is relatively inaccurate and reliance on ultrasound to visualize deep venous clots is the normal standard for diagnosis. Prior to this, clot visualization was performed using x-ray dense contrast and simple repetitive x-rays or fluoroscopic x-ray. Ultrasound is noninvasive quick and very accurate.
Treatment:
Treatment of deep venous thrombosis is best avoided by appropriate prophylaxis. The means for prophylaxis, however, has been controversial for many years. Aspirin was trialed many years ago but in many studies was found to be inferior to Coumadin for deep venous thrombosis prophylaxis. Aspirin was reinitiated more recently but in my experience is convenient but of questionable benefit. Lovenox is an option which is effective however this requires subcutaneous injection twice daily for prophylaxis and is expensive. Coumadin is long-acting, inexpensive, taken once a day and does not require injection. The only downside of Coumadin is monitoring which is generally performed following surgery twice weekly for about 3 weeks. After this time, the risk of deep venous thrombosis is markedly reduced and treatment is discontinued. More modern anticoagulants can be used however these cannot be reversed as Coumadin can, and monitoring cannot be done. Because of this, the risk of bleeding is higher in the perioperative period. It has been my feeling that although Coumadin is more difficult to monitor, the benefits outweigh the inconvenience. It is extremely rare to see a deep venous thrombosis when a patient is on Coumadin and the risk of perioperative bleeding is minimized by maintaining only partial anticoagulation, lower than is used for treatment following a known clot. I have done this successfully for many years and have seen almost no problems. As an Orthopedic Surgeon dedicated to quality care, I follow my own patients and do not defer treatment to their Medical Doctors. I cases where a patient is already on an anticoagulant which cannot be controlled, I suggest switching at least briefly to coumadin which can be controlled, around the time of surgery.
Perioperative Treatment:
Because Coumadin has a 24-hour half-life, (meaning that it is only half gone after a full day), a dose the day before surgery has little or no bleeding risk but is protective. To simplify treatment and cost to the patient, I have given patients Coumadin prior to surgery using a small dose and hopefully enough tablets to fill the 3 weeks following surgery. 3 tablets are given only once on the day before surgery around midday. The size of the tablet for every patient is different depending on weight, age, sex, and a guess of nutritional status. When the patient is in the hospital, they receive a smaller dose the day of surgery and monitoring begins. When the patient goes home, physical therapy and a home care nurse visits 2 or 3 times a week, and they can obtain a PT–INR to monitor the Coumadin effect. This needs to be reported to us so any alteration in the dose can be made. With small tablets given prior to surgery, patients generally take 2 or 3 tablets daily until 3 weeks have completed. Following this, there is no need for monitoring of PT–INR.
Summary:
Deep venous thrombosis is a potentially serious complication which can result from lower extremity fracture, surgery or trauma. The best treatment is to avoid the complication by prophylactic treatment. It has been my experience that Coumadin is effective and very safe when monitored appropriately.
Blood work results (PT–INR) should be faxed to our office at 401-383-8982. If there is any question, please do not hesitate to call the office at 401-383-7753.
Compliments of Sports Medicine and Orthopaedics, East Providence Rhode Island